¿Infarto de miocardio con arterias coronarias permeables?
- amplia2mente
- 1 oct 2018
- 5 min de lectura

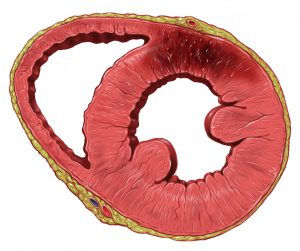
Infarto de Miocardio en la pared anterior del ventrículo izquierdo con arterias coronarias permeables (by Patrick Lynch)
Muchas de las autopsias que se practican en nuestros Institutos de Medicina Legal tienen como causa una cardiopatía, habitualmente una cardiopatía isquémica. En la mayoría de las ocasiones la relacionamos con una enfermedad arterosclerótica en las grandes arterias coronarias con estenosis de su luz, en ocasiones superiores al 75% de la misma. Sin embargo, en las últimas semanas hemos podido comprobar como han surgido varios artículos que indicarían que no siempre esto es así.
Myocardial infarction with permeable coronary arteries?
Many of the autopsies that we practiced in our Institutes of Legal Medicine are caused by heart disease, usually ischemic heart disease. In the majority of the occasions we associate it with an atherosclerotic disease in the great coronary arteries with stenosis of its light, sometimes greater than 75% of them. However, in recent weeks we have seen how some articles have appeared that would indicate that this is not always the case.
El Infarto agudo de miocardio (IAM) sin enfermedad coronaria aterosclerótica obstructiva o MINOCA (acrónimo inglés de Myocardial Infarction With no Obstructive Coronary Aterosclerosis) es un síndrome frecuente en la práctica clínica, ya que supone del 5 al 25% de todos los IAM. Se caracteriza porque en la angiografía, las arterias coronarias son normales o «casi» normales (estenosis angiográficas <50%). Sus causas son múltiples y pueden dividirse en epicárdicas (trombos o espasmos coronarios) y microvasculares (espasmo microvascular, microembolismos, miocarditis o Sdr. Takotsubo).
Acute myocardial infarction (AMI) without obstructive atherosclerotic coronary disease or MINOCA (Myocardial Infarction With no Obstructive Coronary Atherosclerosis) is a frequent syndrome in clinical practice, since it accounts for 5 to 25% of all AMI. It is characterized because in angiography, the coronary arteries are normal or «almost» normal (angiographic stenosis <50%). Its causes are multiple and can be divided into epicardial (thrombi or coronary spasm) and microvascular (microvascular spasm, microembolism, myocarditis or Sdr. Takotsubo).
En un principio se pensaba que al estar las arterias coronarias libres, su pronóstico era mejor, sin embargo no es tan «benigno» como se pensaba y depende en gran medida de la etiología y las alteraciones cardíacas asociadas. Globalmente se ha descrito una tasa de mortalidad por todas las causas durante la hospitalización y a los 12 meses de entre el 0,1-2,2% y 2,2-4,7%, respectivamente. Debido a esto pensamos que los Médicos Forenses que nos dedicamos a la patología forense deberíamos de conocerlos, ya que los pacientes con MINOCA, en particular aquellos con arterias coronarias angiográficamente normales, con frecuencia son etiquetados como «pacientes no cardíacos», perdiendo así la oportunidad de tratar adecuadamente a estos pacientes con un resultado peor de lo que se creía anteriormente y ante la ausencia de tratamiento pueden fallecer ser motivo de denuncia por mala praxis médica.
Initially it was thought that since the coronary arteries were free, their prognosis was better, however it is not as «benign» as was thought and depends largely on the etiology and the associated cardiac alterations. Overall, a mortality rate has been described for all causes during hospitalization and at 12 months between 0.1-2.2% and 2.2-4.7%, respectively. Because of this, we think that Forensic Doctors dedicated to forensic pathology should know them, since patients with MINOCA, particularly those with angiographically normal coronary arteries, are often labeled as «non-cardiac patients», thus losing the opportunity of adequately treating these patients with a worse result than previously believed and, in the absence of treatment, they may die as a reason for reporting medical malpractice.
El primero de los artículos que hemos encontrado en los últimos meses es el publicado por la European Heart Journal titulado «Impact of inflammatory conditions in myocardial infarction with non-obstructive coronary arteries«. En dicho artículo se analiza la relación entre las condiciones proinflamatoris y el MINOCA, así como el impacto de su pronóstico en función de las condiciones inflamatorios. La inflamación crónica causa y acelera muchas enfermedades. Aunque se desconocen varios aspectos de las causas de este síndrome, los autores indican como algunos mediadores de la inflamación van a poder ser responsables de este síndrome.
The first of the articles that we have found in recent months is the one published by the European Heart Journal entitled «Impact of inflammatory conditions in myocardial infarction with non-obstructive coronary arteries«. This article analyzes the relationship between proinflammatory conditions and MINOCA, as well as the impact of its prognosis in terms of inflammatory conditions. Chronic inflammation causes and accelerates many diseases. Although several aspects of the causes of this syndrome are unknown, the authors indicate how some mediators of inflammation will be responsible for this syndrome.
En la revista Circulation, se publicó hace unos meses el artículo «Myocardial Infarction With Nonobstructive Coronary Arteries (MINOCA) The Past, Present, and Future Management» en la que los autores plantean que es el MINOCA pero además hablan de lo que hasta ahora conocíamos de este síndrome, lo que se está haciendo en la actualidad y, quizás lo más importante, el futuro de este cuadro, ya que el término MINOCA sería un concepto demasiado amplio y deberían de utilizarse una nueva nomenclatura reemplazandola por otras denominaciones más específicas (por ejemplo: Arterias coronarias no obstructivas con troponina positiva [TP-NOCA]) que indicaría cuadros de isquemia con troponina positiva y coronarias permeables.
In the magazine Circulation, the article «Myocardial Infarction With Nonobstructive Coronary Arteries (MINOCA) The Past, Present, and Future Management» was published a few months ago in which the authors state that it is the MINOCA but they also talk about what we knew so far of this syndrome, what is being done nowadays and, perhaps most importantly, the future of this table, since the term MINOCA would be too broad a concept and a new nomenclature should be used replacing it with other more specific denominations (for example: Non-obstructive coronary arteries with positive troponin [TP-NOCA]) that would indicate ischemia with positive troponin and permeable coronary arteries.
Muchas de las investigaciones actuales están orientadas al estudio del posible papel de los polimorfismos de los receptores de plaquetas («Myocardial infarction before and after the age of 45: Possible role of platelet receptor polymorphisms«) como causa principal del MINOCA y además orientadas estas investigaciones a posibles tratamientos, basados en los antiagregantes plaquetarios («Dual anti-platelet therapy in myocardial infarction with non-obstructive coronary artery disease«).
Many of the current investigations are oriented to the study of the possible role of platelet receptor polymorphisms («Myocardial infarction before and after the age of 45: Possible role of platelet receptor polymorphisms«) as the main cause of MINOCA and also oriented these investigations to possible treatments, based on platelet antiaggregants («Dual anti-platelet therapy in myocardial infarction with non-obstructive coronary artery disease«).
As we can see, a new concept opens up that may prevent us from discarding myocardial ischemias if the coronary arteries are permeable and therefore adding the MINOCA as the cause of our deaths. We will continue alert to the evolution of this concept.
Como vemos se abre ante nosotros un nuevo concepto que puede hacer que no descartemos isquemias miocárdicas si las coronarias son permeables y por tanto añadir el MINOCA como causa de nuestras muertes. Seguiremos atentos a la evolución de este concepto.



Comentarios